So with all this on my mind, Audrey was admitted on Monday for two days of "cleanout." She could not even tolerate this so it was quickly scrapped. She hasn't been fed in 4 months, how much stool could there be? Wednesday she went to the OR to place the motility probes. They pulled out her GJ tube (which we did not anticipate and it was only 2 weeks old!) and fed a catheter into her jejunum. The catheter has the pressure sensors on then every few cms. They run water through the sensors so as the intestines move, the water is moved and the pressure is measured. Then they placed the same type of catheter (only much longer) into her colon all the way through to where the small intestine and large intestine meet (the cecum for those who know). Each catheter has 8 probes so a total of 16 probes were measuring her activity. She came back to her room and was hooked up to the machine by the GI nurse who stayed with her all day. For 4 hours they just monitor her. This is the "fasting" state. What her intestines do when shes not being fed. At hour 4 she was given IV erythromycin which makes the stomach contract. At hour 5 she was supposed to be fed 8 ounces of formula in 30 minutes in her stomach. This was a huge problem since Audrey has not once in her life consumed 8 ounces at one time, hasn't had feeds at all in 4 months and hasn't tolerated feeds in her stomach for the last 18 months. We comprised to see "as much as she could tolerate." This ended up being 4 ounces in 30 minutes. She was very uncomfortable, nauseous and in pain at this point. At hour 6, a bisacodyl enema was given through the colon probe. We suspected this would work well since this was her home regimen. Sure enough with in 30 minutes her intestines moved. Unfortunately she vomited all of the formula we had given her one hour and a half before and then some. Thankfully at this point the test was over. Now I had to anxiously wait till Thursday to get the results back. Here are some pictures:
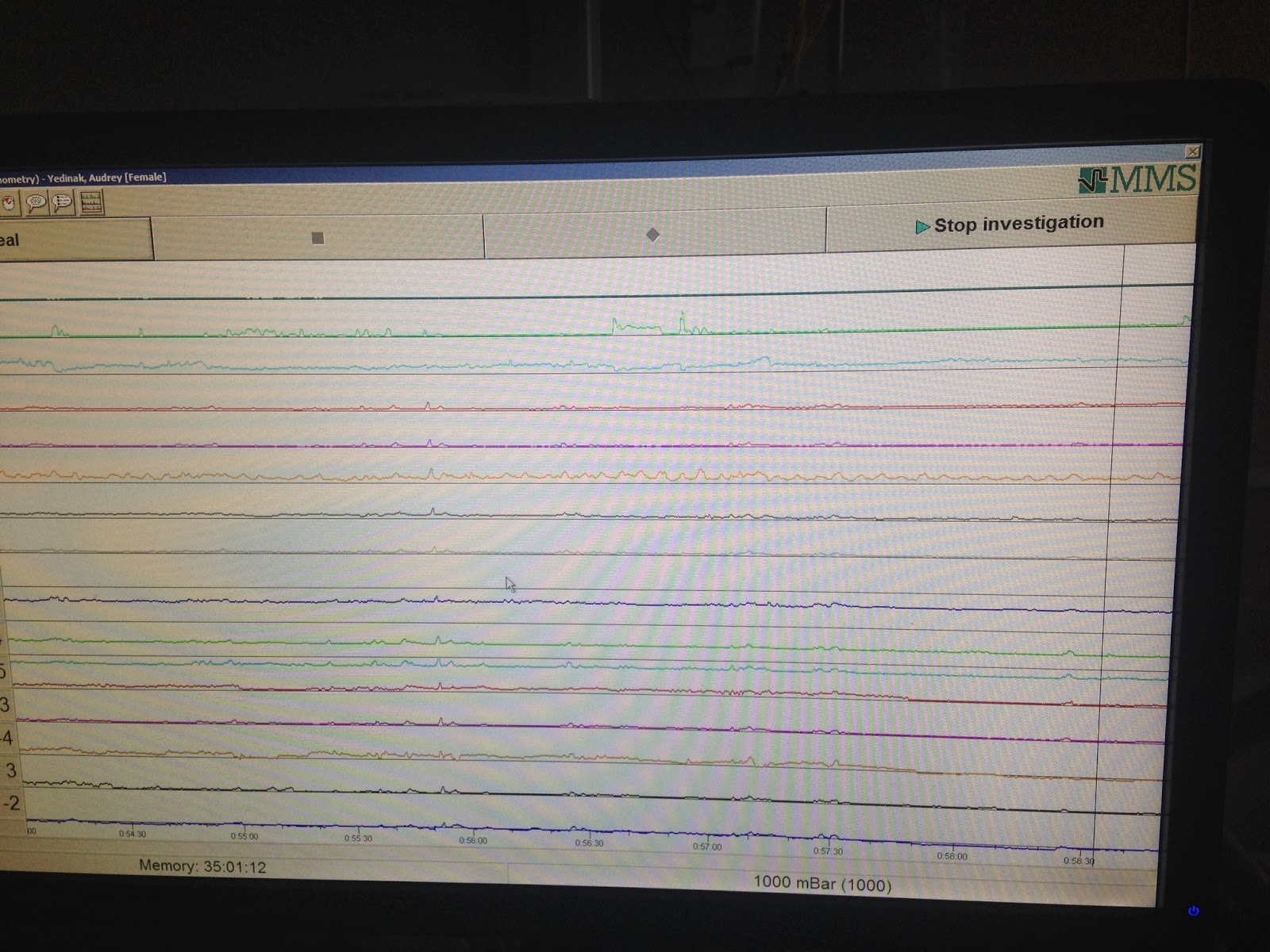


Yesterday the motility doctor and her GI doctor came to speak with me about the results. What they found was on its her intestines did very little moving. As you can see in the graph above. Thankfully her stomach did respond to the IV erythromycin and there were a few contractions made into her small bowel from that. Feeding her did not make her intestines do anything at all. The bisacodyl showed the only the very proximal part of her large intestine has movement. The distal part (the descending colon) had no movement ever. Normally the recommendation is for a distal colectomy but Audrey has mitochondrial disease. This is a progressive disease. Cutting out the piece that doesn't work may help right now but in 6 months or 12 months she may need more out and more out. We just don't know. The next option is to do a c-tube. This is where they place a button in the very begining of her large intestine which does have a little movement and through there we can do the enema flushes. This is not a long term option because we know at some point this will stop working. Our last option is to do an ileostomy. This is where we stop using her colon completely and let her stool out from her small intestine. They also found that her g-tube is located too close to the exit of her stomach. This may be contributing to her pain and may be blocking her stomach. The hope is by relieving the "downstream" obstruction in her colon, her stomach and small intestines will function "normally."
This is very hard news to hear. Though I was expecting her to have poor motility. Being told that she will keep losing what little response she has now is heartbreaking. Having to make these decision is impossible. What if it's the wrong decision? What if it only causes her more pain and suffering? With every step we take with Audrey, I am constantly weighing her quality of life. Right now the has spent 3 of the past 4 weeks in the hospital and the one week she was home her stomach was huge and she was getting around the clock pain medicine. So something needs to happen. The plan is now to move forward with the g-tube relocation and to place the c-tube. I am not ready for the colectomy and I don't think she is ready for the ileostomy. Ultimately we may end up doing one or both, I may end up regretting the c-tube. But this is the least invasive we can be with her at this time and I hope that this will buy us time to come up with a better solution for her. I have no illusions that this will fix anything or make her better. But I hope this will make her more comfortable and keep her out of the hospital for longer periods of time.
No comments:
Post a Comment